The literature on COVID-19 and children is evolving fast. Future versions of this article will reflect updated studies.
Key messages:
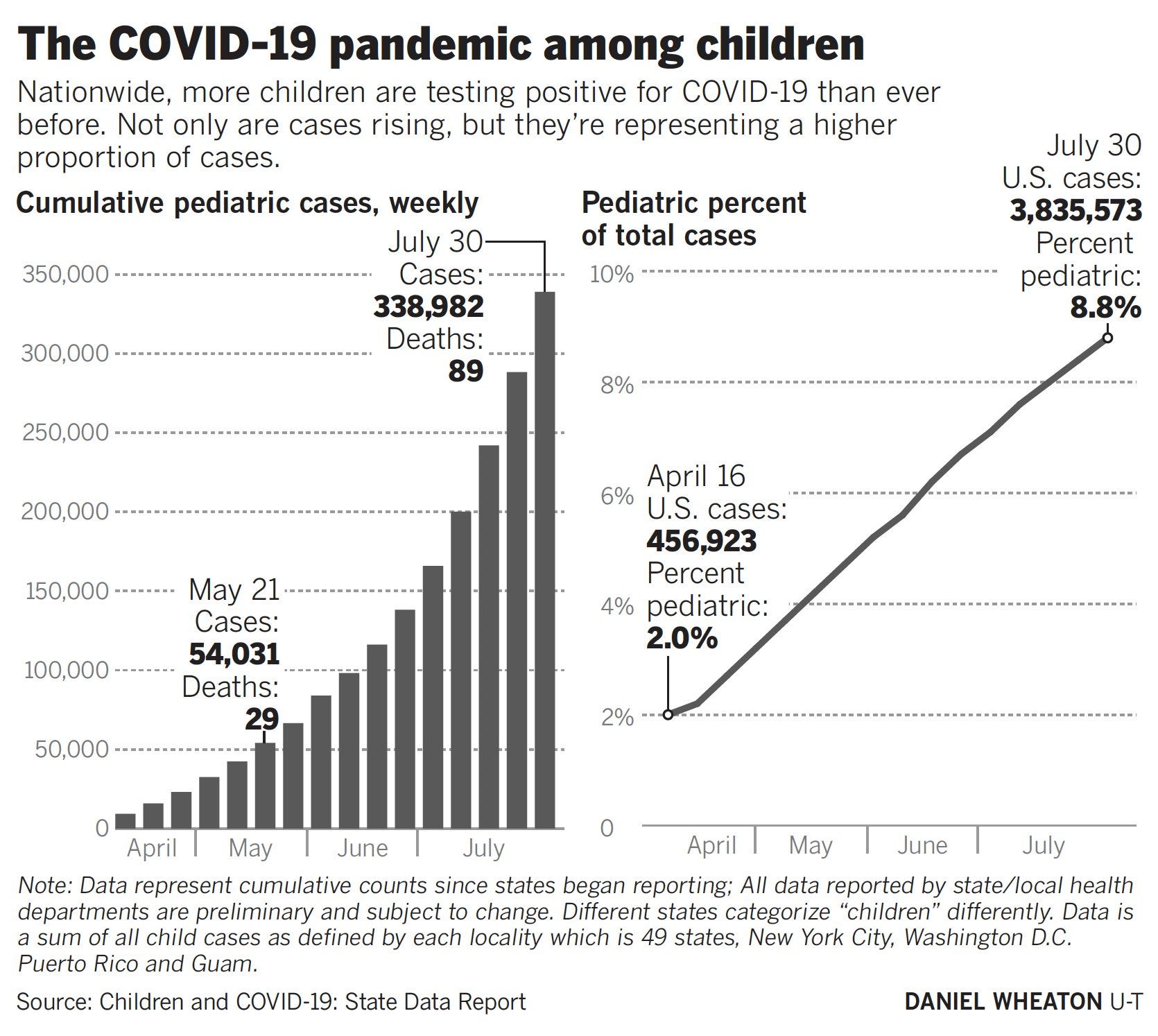
- Children represent an estimated 3–9% of COVID-19 infections. Although children have less severe COVID-19 symptoms than adults, why some children get sicker and a rare few die is still unknown.
- Children transmit COVID-19 to household and non-household contacts with resulting severe outcomes, such as death. Expectant mothers infected with COVID-19 tend to have more severe outcomes than other women of reproductive age. These represent another at-risk cohort in families of school-aged children.
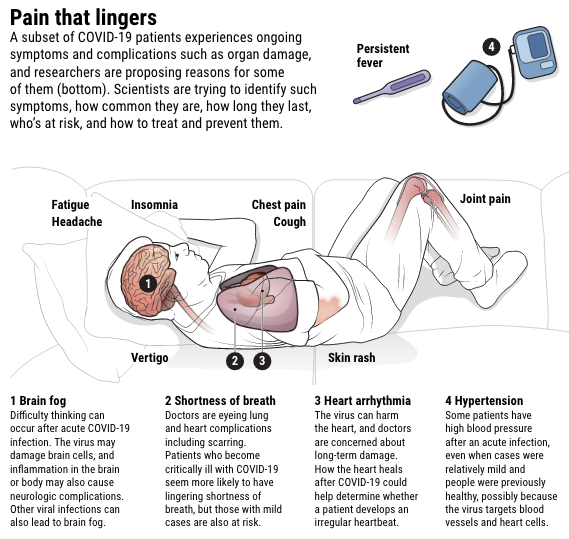
- Long-term effects or “Long COVID”, reported by 10–15% of infected patients, represents a long-term source of disability for family members and school staff. It is too early to document long-term effects on child development, as this is our first year of COVID-19. Masks represent a precautionary public health measure as we learn more about COVID-19.
- Masks are especially useful in schools, which violate the 3C’s of avoiding COVID-19: they are closed spaces with poor ventilation, crowded and involve close contact. Face coverings or masks are the most inexpensive method of breaking the chain of transmission by respiratory droplets in the air. Young children, who are not adept at distancing, will especially benefit from this.
- Parents and teachers can teach children to wear masks using the 4 P’s: play, practice, preparation and patience. Having a comfortable, well-fitting mask is crucial for daily use over hours.
- Masks are one of many pieces in a comprehensive strategy for safe schools, including low community transmission, distancing, hand hygiene, and improved surveillance.
Canadians are still fraught over mask-wearing in our schools. We argue about culture, childrens’ comfort and if kids are the safer for it. The American Academy of Pediatrics now recommends masks for children aged two or older. However, many Canadian provinces have yet to mandate masks in classrooms (e.g. as of this writing BC, almost all Alberta, Ontario for JK-Grade 3). As a data scientist and a physician looking at the evidence (also both parents of school-aged children), we believe the lack of a mask policy for K-12 misses the big picture about a low-cost, low harm, high benefit public health measure that allows exemptions, and will make school reopening safer.
Kids Do Get Infected with COVID-19, Do Transmit To Family, and Can Have Severe Outcomes
Current evidence from research studies and school outbreaks are good enough to mandate face coverings for all Canadian schools. Seroprevalence and epidemiological studies show that children comprise 3% to 9% of infected cases in a population. Epidemiologists caution that early estimates of infection rates in children may be artificially low due to school closures in the Spring and early testing limited to severe cases. Children tend to be asymptomatic or have less severe symptoms (but not always), and death is rare.

Tracing of ~59,000 contacts of ~5,700 cases in South Korea found that children of all ages transmit COVID-19 to household contacts. Supporting this evidence, a study in Chicago found that nasal swabs from the youngest children contained more viral DNA than those from adults. Larger outbreaks in US camps and Israeli schools have infected hundreds of staff and students, sometimes largely children under the age of 10. Israel’s largest school outbreak occurred after mandatory masking was relaxed because of a heat wave. More recently one kindergarten teacher died. We’ve had outbreaks in Canada too. A child infected 9 out of 11 children in a Trois-Rivières elementary classroom. A summer school in Calgary had small class sizes and distancing but still reported one infected teacher and student, after its first student case; three children under 12 were infected in a daycare outbreak in Calgary this month.
Another risk factor for young families is the impact of the illness on expectant mothers. In a study with 91,000 COVID-positive women of reproductive age, CDC reports that pregnant women are 1.5 times more likely to be admitted to the ICU and 1.7 times more likely to need ventilators. Although this study used only data for women for whom pregnancy status was available, it is an indication of increased disease severity in pregnancy. A much smaller study in Sweden found a similar trend.
So the health risks are real.
Long-term Effects
Emerging research from the UK, Italy, and Germany have shown that patients have symptoms such as fatigue, shortness of breath, headaches, and concentration difficulties, that negatively impact quality of life even 8-12 weeks after diagnosis with COVID-19. This is supported with formation of online support groups for patients who are suffering long-term symptoms. 10–15% of COVID-19 survivors are “long-haulers”, who suffer from debilitating symptoms over three months after contracting the illness, including heart damage, extreme fatigue, and brain fog. We don’t yet have enough data or time to know if there is long-term (permanent) organ damage from COVID-19, but must be alert to this potential. In fact, two recent studies reported heart damage months after infection, including 78% of a sample of patients in Germany; alarmingly, a majority of these were never hospitalized and would have been categorized as “mild”. As this is humanity’s first year of COVID-19, we do not yet know what long-term effects this disease has on infected children.

Together, these data pose sobering questions about the suffering and illness that will be caused by school outbreaks to children, staff, teachers and the community. Sure, we can wait for better studies (like we did for our LTC homes), but a face covering is hardly high stakes; why not use the precautionary principle?
School buildings with poor ventilation increase chance of outbreaks
Schools violate the 3C’s of avoiding COVID-19: They are closed spaces with poor ventilation, crowded places, and involve close contact. As more large municipalities mandate masks in indoor spaces — Toronto, Ottawa, Montreal, Edmonton, Calgary and Halifax — , schools remain a bizarre exception to this new norm. The majority of Canadians want staff and students to be masked at school. In most of Ontario, kids under 10 will mask up in all indoor places, except for schools. Shunning masks is unwise as developmentally, this cohort will have the most difficulty with hand hygiene and distancing. As Ontario teachers would be more protected in a nail salon, no wonder less than half of Toronto teachers are comfortable returning to school. BC’s plan is worse than Ontario’s, as it only mandates masks in hallways and not classrooms. A mask mandate will allow for those who must be exempt for developmental, behavioural or medical reasons to safely opt out, but still be reasonably protected if the majority of their peers mask. A mask mandate for students and staff will make schools safer for everyone.
Masking is achievable with comfortable masks and the 4P’s: play, practice, preparation and patience


Children are more adaptable than we realize. Schools in Germany, South Africa, and South Korea have successfully mandated masks. We teach our children to cover their mouths when they sneeze, and to wash hands after using the toilet. Similarly, safe mask-wearing can be taught using the 4 Ps: play, practice, preparation, patience. These can be done with parents and teachers, educational posters, and reinforcement. For improved adoption, children can create colourful custom masks.
Parents and children need to work together to find a well-fitting, comfortable mask. Toronto Public Health recommends a two-layer fabric mask that maintains its shape after washing(cotton/polyester). Masks with exhalation valves let out infectious particles and are not recommended. For younger children, ear-loops are better than fabric ties; ear-savers or over-the-head elastic designs can avoid chaffing the ears from prolonged use. The mask must fit snugly with no gaps around the face.
Masks are one piece of a larger, comprehensive strategy of infection control for safer schools

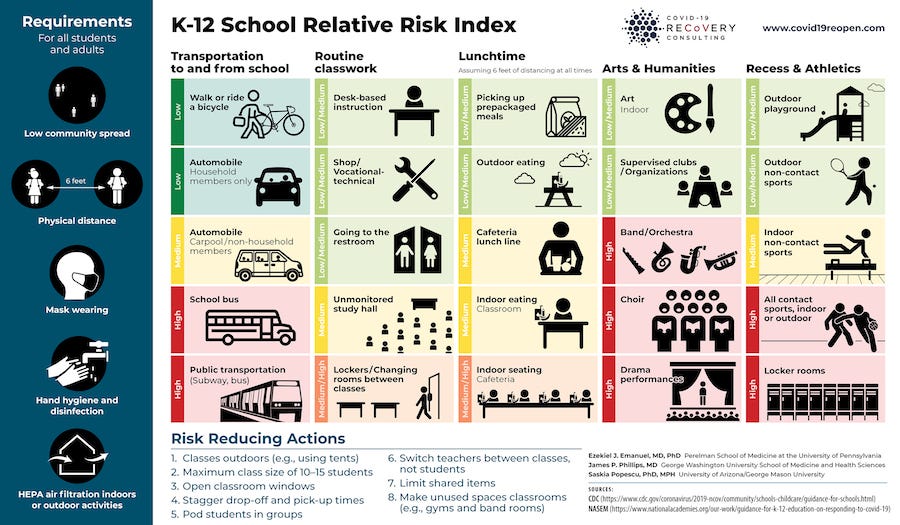
The start of school is a community ritual of reunion and growth. A safe school reopening includes several important pieces (also see this), including low community transmission, paid sick leave, distancing, hand hygiene and PPE, improved ventilation, improved testing, and limited student and staff mobility. The data are clear: Masks are the “low-hanging fruit” of infection control that will help limit outbreaks at schools and help rebuild the economy with more peace of mind. Schools will remain open for longer, providing equitable access to education and childcare. To reopen schools without mandating masks for all children, staff and visitors would be unconscionable recklessness.
Dr. Shraddha Pai, PhD uses data science for genomic medicine, and is a mother of two children in elementary and middle school in Toronto. Dr. Pai is a Postdoctoral Fellow at the Donnelly Centre for Cellular and Biomolecular Research and University of Toronto. Dr. Amy Tan, MD, MSc is a family physician and researcher and associate professor of family medicine at the University of Calgary and is a mother of one elementary-aged child. Drs. Pai and Tan are both supporters of non-medical masks, and are members of the grassroots advocacy group Masks4Canada (masks4canada.org).